36 year old male with DKA with anemia
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome .
I’ve been given this case to solve in an attempt to understand the topic of “patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan.
Case:
34 year old male c/o swelling of swelling of left leg since 2 months
Decreased pedal edema since 15 days
Decreased urine output since 15 days
Headache since evening
HOPI:
Pt was apparently asymptomatic 2 months back then he was hit with a rock on left foot then he developed swelling of leg since then
Fasciotomy done 15 days back
Since then he developed pedal edema and there was decreased urine output




Past history:
K/c/o DM since 10 years
Diabetic history:
10 years back he had fever for which he went to local hospital and got tested and found that his blood sugars were 560mg/dl and was prescribed with glucoryl m1 for 5 years then switched to insulin on advice of local doctor which he takes according to the food intake as 5-10 units of insulin by himself he gets his sugars checked every month and adjusts the dose of insulin accordingly
Not a k/c/o HTN, TB, asthma , CAD , epilepsy
Personal history:
Auto driver by occupation
Diet: mixed
Appetite: normal
Bowel and bladder habits: regular
Allergies: none
Addictions: none
Family history: insignificant
General examination:
Pt is conscious,coherent and cooperative
Well oriented to time , place and person
Moderately built and nourished
Pallor and pedal edema ( pitting type)
Icterus, cyanosis, lymphadenopathy are absent
Vitals:
Temp: afebrile
BP: 130/80 mm Hg
PR: 112bpm
RR: 24 /min
GRBS: 332mg/dl
Systemic examination:
CVS: s1, s2 heard
No murmurs
RS: BAE+
CNS: no focal neurological deficits
Per abdomen:
On inspection:
Shape - scaphoid
Abdomen moves equally with respiration.
Umbilicus inverted
No scars and sinuses present.
No visible pulsatios , no engorged veins
On palpation:
No tenderness
No rebound tenderness, no gaurding, no rigidity
No organonegaly
On percussion:
No fluid thrill
No shifting dullness
On Auscultation:
Bowel sounds heard
Investigations:
Hemogram:
On 16-10-2022

On 17-10-2022

On 18-10-2022

On 19-10-2022

Blood grouping and typing:

Peripheral smear :

Reticulocyte count :

APTT:

Prothrombin time:

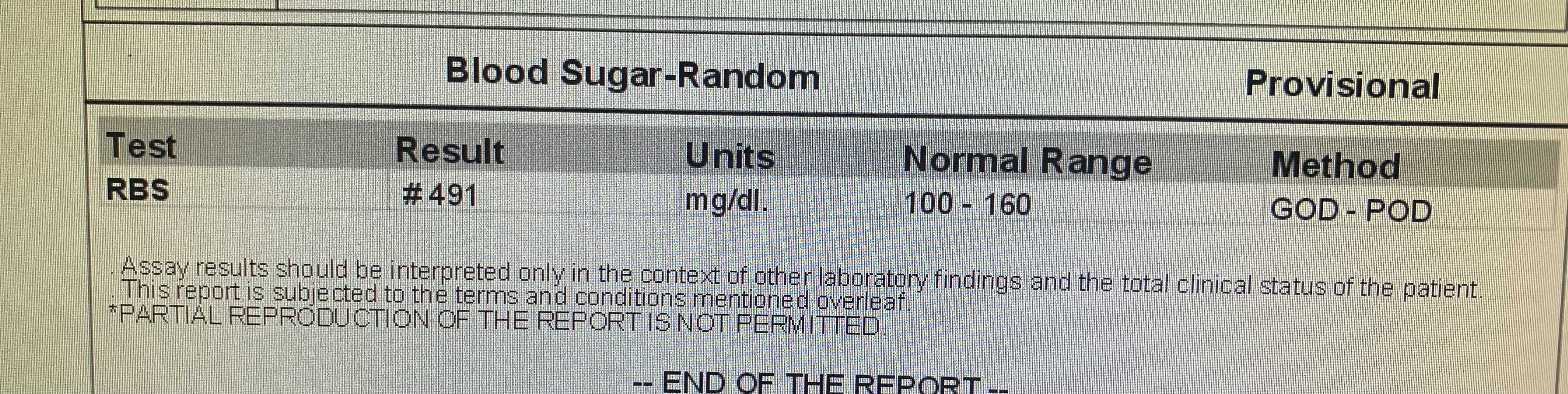
Random blood sugar:
Blood urea :
On 18-10-2022:

19-10-2022:

Urine protein/ creatinine ratio :

LFT:

Serum creatinine :
On 18-10-2022:

On 19-10-2022:

Serum electrolytes:
On 18-10-2022:

On 19-10-2022

Urine for ketone bodies:

Serology: negative
HCV:


Provisional diagnosis:
DKA (resolved ) with anemia
S/p fasciotomy done 15 days back
Treatment:
1) Inj human actrapid insulin 6U /iv /stay
2) Inj human actrapid insulin infusion @ 6 ml /hr
1ml HAI in 39 ml NS
3) iv fluids 1NS @75ml /hr



Comments
Post a Comment